Case: A 50 year old male with alcohol abuse present in the Emergency department with mild chest pain. He has been nautious and vomiting the past couple of days. Also there is diffuse abdominal tenderness. He gets admitted to control pain and CT-scan next days but detiorates suddenly. He dies. Obduction shows a ruptured oesophagus.
Boerhaave syndrome is rupture of esophagus and rapidly fatal.
History: a dutch grand admiral was retching and tore his oesophagus apart. He died after eating a duck.
Pathofysiolygy: rupture of esophagus due to increase intraluminal pressure usual due to vomiting or retching. Alcohol intake is related. Higher risk if gastro-intestinal disease is present.
Other causes: straining, childbirth, heavy lifting, seizures, fits of coughing or hiccup
Clinical symptoms: chest pain, nautious, vomiting (bloody), dysphagia, dyspnea,
Anderson Triad: Subcutaneous emphysema, rapid respirations, and abdominal rigidity
Macler triad: vomiting, pain, subcutaneous emphysema
Physical examination: Crepitus in the neck, abdominal rigidity, abdominial pain. tachycardia, tachypnoe
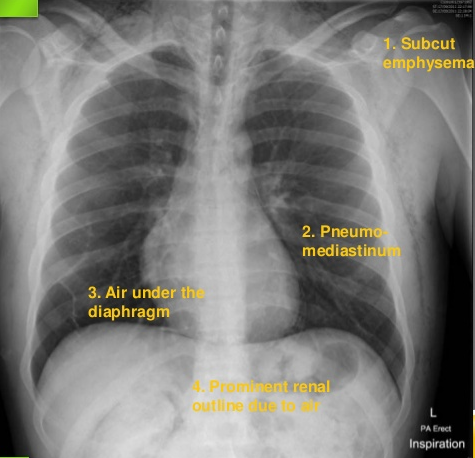
Chest X-ray signs:
- Subcuteneous emphysema
- Pneumomediastinum
- Free air under the diaphragm
- Pleural fluid
If still suspected make CT-thorax/abdomen (contrast in esophagus?).
Treatment:
* Surgery as soon as possible
Aggresive resuscitation and broadspectrum antibiotics.
The cause of death is usually polymicrobial septic shock and mediastinitis.




